


Moxibustion for breech babies - Wokingham, Berkshire
On this page
- Overview
- What is a breech presentation?
- What is moxibustion and how does it work for breech?
- Research evidence
- When to start moxibustion
- How to apply moxibustion at home
- When to avoid moxibustion
- Other techniques to help turn a breech baby
- Treatment at my clinic
- Frequently asked questions
- References
1. Overview
A breech presentation — where the baby lies bottom-down rather than head-down in the womb approaching the end of pregnancy — affects approximately 3–4% of pregnancies at term. When a baby remains in a breech position at 36 weeks, most UK hospitals will discuss external cephalic version (ECV) — a procedure in which a clinician manually attempts to turn the baby from outside the abdomen — or plan for a caesarean section. Both carry their own risks and are not always the preferred option for expectant mothers.
Moxibustion — a traditional Chinese technique involving the burning of dried mugwort (moxa) near a specific acupuncture point on the little toe — has been used in China for over two thousand years to encourage a breech baby to turn to a head-down position. It is safe, non-invasive and can be self-administered at home by the mother or a partner after professional instruction. A growing body of clinical research including a Cochrane systematic review confirms that moxibustion combined with usual care probably reduces the number of non-cephalic (breech) presentations at birth. I offer moxibustion for breech presentation at my clinic in Wokingham, Berkshire, and teach expectant mothers the home technique during their appointment.
2. What is a breech presentation?
In a normal (cephalic) presentation, the baby lies head-down in the uterus from around 28–32 weeks of pregnancy, ready for birth with the head as the leading part. In a breech presentation, the baby is positioned with its bottom, feet or knees facing downward instead.
There are three main types of breech presentation:
- Frank (extended) breech — the most common type, where the baby’s bottom presents first with both legs stretched upward alongside the body and feet near the head
- Complete (flexed) breech — the baby sits cross-legged, with bottom down and both knees bent
- Footling (incomplete) breech — one or both feet are the presenting part below the bottom
Most babies naturally turn head-down by 36 weeks. If a breech presentation persists beyond 36 weeks it is worth exploring all available options, including moxibustion, before proceeding to ECV or planning a caesarean section. Moxibustion is most effective when started earlier — ideally between 33 and 36 weeks — giving the baby more room to turn.
3. What is moxibustion and how does it work for breech?
Moxibustion involves burning a stick or cone made from dried mugwort leaves (Artemisia argyi or vulgaris, known in Chinese as Ai Ye) close to the skin at a specific acupuncture point, without direct contact. The gentle, penetrating warmth generated is thought to stimulate the body’s energy channels and promote physiological responses in the uterus.
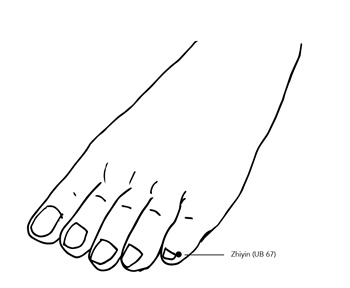
For breech presentation, the specific point used is BL67 (Bladder 67, known as Zhiyin), located at the outer corner of the nail of the little toe on each foot. BL67 is the terminal point of the Urinary Bladder channel, one of the longest meridians in the body, which runs along the back of the leg and through the uterus and lower back. In traditional Chinese medicine (TCM), stimulating BL67 with warmth is believed to tonify the Yang energy of the Urinary Bladder channel, increase uterine activity and fetal movement, and activate the body’s natural mechanisms to encourage the baby into an optimal position for birth.
From a biomedical perspective, the proposed mechanisms by which moxibustion at BL67 may encourage cephalic version include:
- Stimulation of placental oestrogen and prostaglandin release, which increase uterine contractility and fetal movement
- Direct activation of adrenocortical hormones, increasing uterine activity
- Enhancement of blood circulation to the uterus
- Increased fetal motor activity via thermal and neurological stimulation, which encourages the baby to reposition spontaneously
4. Research evidence
The evidence base for moxibustion at BL67 for breech presentation has grown substantially over the past two decades. A Cochrane systematic review by Coyle, Smith & Peat (2023) — the most rigorous and up-to-date review available, evaluating 13 studies involving 2,181 women — found that moxibustion combined with usual care probably reduces the number of non-cephalic presentations at birth compared with usual care alone or sham moxibustion, with moderate-certainty evidence. The review also found that moxibustion combined with usual care probably reduces the need for oxytocin during labour. A systematic review and meta-analysis by Liao et al. (2021), published in Healthcare, included 16 RCTs with 2,555 participants and found that moxibustion significantly increased cephalic presentation at birth (risk ratio 1.39; 95% CI 1.21–1.58), with the effect present in both Asian and non-Asian populations. A systematic review by Vas et al. (2009), published in the American Journal of Obstetrics and Gynecology, found moxibustion significantly favoured correction of non-vertex presentation at delivery (RR 1.29; 95% CI 1.12–1.49). An RCT by Brici et al. (2019) published in Evidence-Based Complementary and Alternative Medicine confirmed the effectiveness of moxibustion and acupuncture for turning breech babies at 32–35 weeks gestation. Research also confirms the cost-effectiveness of moxibustion as a first-line intervention for breech presentation at 33 weeks, with significant savings compared to ECV and caesarean section (van den Berg, 2010).
It is important to note that trial results are mixed — some individual studies have not found a significant effect, particularly in non-Asian populations. However, the weight of evidence from systematic reviews and meta-analyses across thousands of participants supports moxibustion as a safe and potentially effective natural option that is worth trying before proceeding to more invasive interventions.
5. When to start moxibustion
Timing is important for moxibustion to work effectively for breech presentation:
- Ideal window: 33–36 weeks — starting between 33 and 36 weeks gives the baby the most space and time to turn. The earlier in this window treatment begins, the more flexibility the baby has to move. Most research protocols begin treatment at 33–35 weeks
- Still worth trying from 36–39 weeks — while the window is narrower and the baby has less room to turn, moxibustion can still be attempted at up to 39 weeks alongside medical assessment and planning
- Confirm breech position first — before beginning moxibustion, the breech presentation should be confirmed by your midwife or via ultrasound scan. Moxibustion should not be used if the baby has already turned head-down
- Confirm normal position of placenta — placenta praevia (low-lying placenta) is a contraindication for any techniques to encourage fetal turning. Ensure this has been assessed by your midwife or obstetrician
6. How to apply moxibustion at home
I recommend that expectant mothers visit the clinic first to have moxibustion performed professionally and to receive proper instruction before self-administering at home. At the appointment, I will demonstrate the correct technique, show you the precise location of BL67, and ensure you are comfortable and confident to continue at home.
Equipment you will need
- A box of smokeless moxa sticks (usually 5 per box, which should be sufficient for a full course of treatment)
- A BBQ lighter or Zippo lighter — a standard household lighter is not recommended as the flame needs to be held for several minutes to light the moxa stick and a regular lighter may overheat
- A small ceramic or glass dish (or ashtray) to hold the moxa stick and catch ash during treatment
- A glass jar with a tight-fitting lid (such as a jam jar) to extinguish the moxa stick safely after treatment
Step-by-step instructions
- Prepare your space — ensure the room is well ventilated (open a window). Sit in a comfortable position with easy access to both little toes. Have your dish and jar within reach before you begin
- Light the moxa stick — hold the tip of the moxa stick in the flame of the lighter for several minutes, blowing gently on the end to get it glowing bright red. Tap off any grey ash into the dish before you begin
- Apply to BL67 — hold the glowing end of the moxa stick approximately 2 cm (1 inch) from the outer corner of the nail of the little toe. Do not allow the stick to touch the skin. Use your other hand to steady the hand holding the moxa stick if needed
- Monitor the heat — the area should feel pleasantly warm but not hot or burning. When it starts to feel uncomfortably hot, move to the other little toe. Keep the end of the moxa stick glowing by blowing gently and removing ash regularly by tapping it into the dish
- Duration — treat each little toe for approximately 20 minutes per session (40 minutes in total across both toes), for 10 consecutive days
- Best time of day — the traditional recommendation is to perform moxibustion between 3 and 5 pm, which corresponds to the peak activity time of the Urinary Bladder channel in the TCM body clock. If this is not practical, consistency of daily treatment is more important than exact timing
- Extinguish safely — at the end of each session, place the moxa stick into the glass jar and screw the lid on firmly to extinguish it. Never leave a burning or smouldering moxa stick unattended
- After turning — if you feel strong fetal movement or suspect the baby may have turned, contact your midwife and arrange an ultrasound to confirm the position. If the baby has turned to cephalic, reduce treatment to 10 minutes per toe and continue until day 10 to help the baby consolidate the new position
7. When to avoid moxibustion
Moxibustion for breech is generally very safe, but should be avoided or used only under close professional guidance in the following situations:
- High-risk pregnancy — including placenta praevia, oligohydramnios (low amniotic fluid), pre-eclampsia, previous uterine surgery (other than routine caesarean section), or any condition your obstetrician has identified as requiring careful monitoring
- Multiple pregnancy — moxibustion for breech is generally intended for singleton pregnancies; discuss with your midwife or obstetrician before using in a twin pregnancy
- Absence of professional instruction — do not attempt moxibustion without first receiving proper training from a qualified practitioner. Improper application can cause burns
- Allergy to smoke or mugwort — if you have asthma or significant respiratory sensitivity, even smokeless moxa sticks may cause irritation. Discuss this with your practitioner before beginning
- Strong fetal movements or discomfort during treatment — if moxibustion causes significant discomfort, strong uterine contractions or reduced fetal movement, discontinue immediately and contact your midwife
Always inform your midwife and obstetric team that you are using moxibustion so that your care can be coordinated appropriately.
8. Other techniques to help turn a breech baby
Moxibustion works best as part of a combined approach. The following techniques are commonly used alongside moxibustion and may increase the likelihood of the baby turning:
- Optimal foetal positioning — spending time on all fours, kneeling with the bottom raised, or reclining on a tilted surface (with hips slightly higher than the shoulders) can use gravity to encourage the baby to move into a better position. The Spinning Babies approach (spinningbabies.com) provides detailed guidance on positioning exercises
- Swimming — time in a swimming pool, particularly floating face-down in the water, gives the baby more room to move and may encourage turning
- Acupuncture at BL67 — acupuncture needling at BL67 can be used alongside moxibustion for additional stimulation of the point. Some research protocols use both together and show enhanced results compared to moxibustion alone
- External cephalic version (ECV) — a medically supervised procedure performed in hospital at around 36 weeks, in which an obstetrician attempts to turn the baby manually. Success rates vary (approximately 50%) and ECV is not suitable for all pregnancies. Moxibustion is often used first, with ECV as the next step if moxibustion has not been successful
9. Treatment at my clinic
I offer moxibustion for breech presentation at my clinic in Wokingham, Berkshire. At the initial appointment, I perform moxibustion professionally at BL67, demonstrate the precise technique and location of the point, and provide full instruction for home self-treatment. I also supply guidance on the optimal timing and duration of home sessions and advise on the supporting positioning techniques.
Treatment is most effective when started between 33 and 36 weeks, though it is worth attempting up to 39 weeks. Most women require one to two clinic appointments for initial treatment and instruction, and then continue the home protocol daily for ten days. Read more about pregnancy treatments I offer and see the prices page for treatment costs. For further reading, I have written a comprehensive self-help guide to healthy pregnancy: My Pregnancy Guide.
10. Frequently asked questions
Does moxibustion really work for turning breech babies?
The evidence is encouraging though not definitive. A 2023 Cochrane systematic review of 13 studies including 2,181 women found that moxibustion combined with usual care probably reduces the chance of non-cephalic presentation at birth, with moderate-certainty evidence. A 2021 meta-analysis of 16 RCTs with 2,555 participants found moxibustion significantly increased cephalic presentation at birth (RR 1.39). Results are more consistent in trials conducted in Asian populations, and individual study results are mixed. The overall picture is that moxibustion is a safe, non-invasive intervention that is well worth trying before more invasive procedures.
When is the best time to start moxibustion for breech?
The ideal window is 33–36 weeks of pregnancy, when the baby still has enough room to turn and moxibustion has the most time to work. It can still be tried between 36 and 39 weeks but is less likely to be effective as the baby has less room to move in the later stages.
Is moxibustion safe in pregnancy?
Yes, when performed correctly by a trained practitioner and self-administered following proper instruction, moxibustion at BL67 is considered safe for most pregnancies. Multiple systematic reviews confirm no significant adverse effects on mother or baby. The main safety consideration is burn risk from improper technique, which is why professional instruction before home use is essential. Smokeless moxa sticks further reduce the smoke exposure associated with traditional moxa.
How long does each moxibustion session take?
Each home session involves applying the moxa stick to each little toe for approximately 20 minutes per foot, for a total of around 40 minutes. Treatment is repeated daily for 10 days. The best time of day is traditionally between 3 and 5 pm, corresponding to the peak activity time of the Urinary Bladder channel, though consistency of daily treatment is more important than exact timing.
What if the baby turns during moxibustion treatment?
If you feel strong fetal movement or suspect the baby has turned, contact your midwife and arrange an ultrasound scan to confirm the position. If the baby has moved to a cephalic (head-down) position, reduce treatment to 10 minutes per toe per session and continue until the tenth day to help the baby remain in the correct position.
Can I combine moxibustion with external cephalic version (ECV)?
Yes. Moxibustion is typically used before ECV as a first-line natural option. If moxibustion has not been successful by 36–37 weeks, ECV can then be considered. Using moxibustion first may also prepare the uterus and improve conditions for a successful ECV if one is subsequently performed. Always coordinate with your midwife or obstetrician when combining approaches.
11. References
Caron J. Breech Presentation. StatPearls Publishing LLC, 2020.
Impey L and Child T. Obstetrics & Gynaecology. Chichester: John Wiley & Sons, 2012.















